Are Your Teeth Secretly Causing Your Headaches?
- drnarayanasaggere
- Jan 25
- 7 min read
Malocclusion, Occlusal Imbalance & Headaches:
A Scientific Insight into Contact Points, TMJ Stress, Masseter Hypertrophy and the Role of T-Scan
Writer: Dr. S. S. Narayana Dental Surgeon | Occlusion • TMD • Airway & Dental Sleep Medicine
Dr. Narayana Dental,
Malkajgiri, Secunderabad
Updated: April 2026
Introduction: Headache disorders are among the most common complaints in general practice and neurology clinics. While migraines, sinus issues, cervical spondylosis, and visual strain are frequently suspected, one major source of chronic pain remains underdiagnosed and underestimated:
Malocclusion and occlusal imbalance—especially wrong contact points created by missing teeth, ill-fitting crowns, faulty bridges, and improper fillings.
In my clinical practice, I often see patients who visit multiple doctors, take pain medications for months or years, and still suffer from:
chronic headaches of unknown origin
temple pain
facial pain mimicking neuralgia
jaw joint (TMJ) discomfort
pain while chewing
tinnitus or ear fullness
neck pain radiating to shoulder region
Many of these patients have a common underlying factor: an unstable bite.
This article aims to explain, in simple but scientific detail:
What occlusion and contact points really mean
How occlusal imbalance affects TMJ and masticatory muscles
Why masseter hypertrophy is a visible sign of overload
How T-Scan has transformed objective occlusal diagnosis
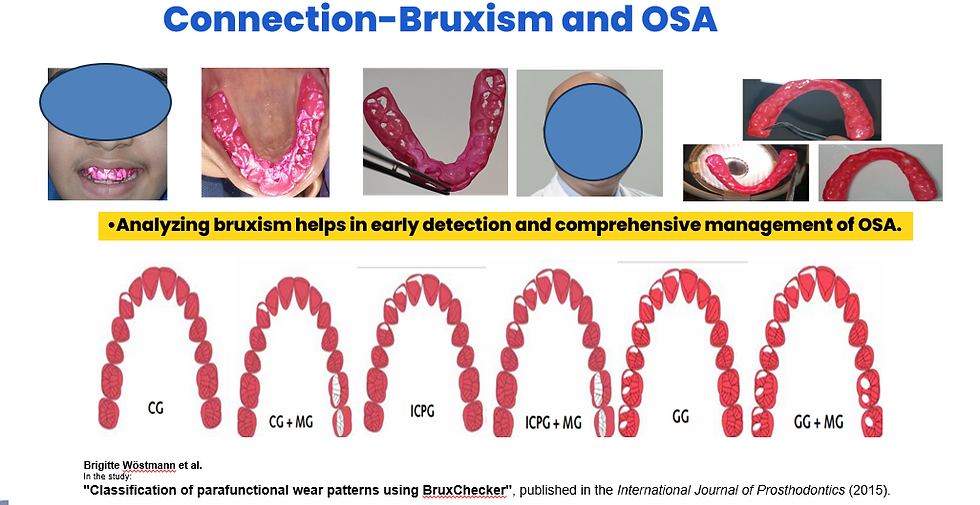
How bite collapse and tooth loss can worsen snoring & OSA
Occlusion: More Than Just Teeth Touching
Occlusion is the manner in which maxillary and mandibular teeth contact each other during:

closure into maximum intercuspation (MIP)
chewing cycles
lateral movements (excursions)
protrusive movements
Occlusion is a neuromuscular event, guided by:
teeth anatomy and proprioception
periodontal ligament feedback
temporomandibular joints
neuromuscular coordination of muscles of mastication
A stable occlusion provides:
✅ posterior support (posterior stops)
✅ anterior guidance
✅ harmonious muscle activity
✅ minimal joint stress
A disturbed occlusion creates:

❌ premature contacts
❌ deflective slides
❌ prolonged clenching reflex
❌ muscle hyperactivity & pain
The Key to Occlusion: First Molars as Functional Pillars
A practical clinical concept that every clinician and patient should understand:
The key to occlusion has much to do with how the maxillary first molar and mandibular first molar come together.
These teeth bear the highest functional load and help maintain:
vertical dimension of occlusion (OVD)
stable mandibular positioning
balanced force distribution
When first molars are restored poorly or lost, the entire occlusion becomes vulnerable to collapse.
Every Tooth Is Anatomically Engineered (Not Flat)
Natural teeth are not flat stones. They are highly engineered structures with:

cusps (functional and nonfunctional)
fossae
grooves
marginal ridges
inclines guiding mandibular movement
Each tooth has unique anatomy and occlusal role. When crowns are fabricated without respecting morphology, the outcome is often:
broad, flat “table-top” occlusal surfaces
inaccurate cusp-fossa relationship
unstable functional occlusion
Occlusal Contact Points: Why “Flat Contacts” Are a Serious Mistake

One of the most common restorative errors I see is this: crowns fabricated with flat contacts, without importance given to morphology, contact points, cusp angulations, or guidance. But occlusion works on precise points, not broad surfaces.
Functional Cusps
Maxillary molars: palatal cusps

Mandibular molars: buccal cusps
These cusps should contact in a precise manner and glide smoothly on inclines of opposing teeth during lateral excursion.
When contact areas become broad and heavy, the closing muscles must recruit more activity for mandibular stability.
Missing Teeth / Worn Dentition = Bite Collapse (Loss of OVD)
What is Bite Collapse?
Bite collapse is commonly called:

Loss of vertical dimension of occlusion (OVD)
Meaning: upper and lower jaws rotate closer than normal.
Major causes
1) Severe bruxism and tooth wear
Occlusal surfaces flatten and shorten due to grinding.

2) Tooth loss and posterior collapse
When multiple teeth are missing, remaining teeth tip, migrate, and overload.
How Malocclusion Causes Headaches, Facial Pain and Neuralgias
When a person closes into MIP, the mandible should stop with minimal interference. But when occlusion is disturbed:
one tooth hits first (prematurity)
mandible shifts to find stability
muscles contract forcefully to “hold” the jaw
This triggers:
1) Muscle hyperactivity
Primarily:
masseter
temporalis
medial pterygoid
2) TMJ strain
Deflective shifts can compress TMJ structures, increasing loading forces.

3) Referred pain
Pain can refer to:
temporal region
maxillary region
ear region
cervical region (C2–C3 nerve branches)
This is why patients describe:
“Doctor, I feel pain in my head, not in teeth.”
Indeed—occlusal pain often manifests as headache.
Masseter Hypertrophy: A Visible Clue of Chronic Occlusal Overload
A clinically powerful but often ignored sign is:
masseter hypertrophy


Masseter hypertrophy means enlargement of masseter muscle due to chronic overuse, commonly caused by:
bruxism
clenching
unilateral chewing
premature occlusal contacts
faulty restorations/crowns
Why is it important?
Because it indicates:
high bite forces
prolonged muscular contraction
imbalance between left and right muscles
Associated complaints
cheek pain
jaw tightness
morning stiffness
temporal headaches
facial asymmetry / squarish lower face
TMD symptoms
The Role of T-Scan: Objective Occlusal Diagnosis (Beyond Articulating Paper)
Traditional occlusal assessment includes:
articulating paper marks
shimstock pull test
patient’s “feel of high point”
But these are subjective.
The critical truth
Articulating paper shows where teeth touch, but it does NOT accurately show:
which tooth touched first
timing sequence of occlusal contacts
percentage force distribution
overload side
occlusion/disclusion timing
This is where T-Scan becomes revolutionary.

T-Scan is like an ECG for occlusion.😊
It provides quantitative digital evidence of occlusal dynamics.
T-Scan Parameters That Matter Clinically
✅ 1) Force distribution (%)

Shows left vs right balance.
Imbalance correlates with:
unilateral clenching
muscle hypertrophy
TMJ loading
✅ 2) First contact identification
Helps detect premature contacts that trigger neuromuscular reflex.
✅ 3) Occlusion Time (OT)
Time taken from initial tooth contact to full intercuspation.
Prolonged OT → increased muscle activity
increased strain → headache, muscle fatigue
✅ 4) Disclusion Time (DT)
Time required to separate posterior teeth during excursions.
A prolonged DT is strongly associated with:
muscle hyperactivity (temporalis/masseter)
myofascial pain

chronic tension-type headache
TMD symptoms
Occlusal imbalance can displace mandibular position and shift TMJ loading. This can manifest as:
TMJ arthralgia (joint pain)
clicking
restriction
discomfort during chewing
Pain may even radiate to cervical region via muscle chains and nerve pathways.
Thus, bite imbalance is not just dental—it is a craniofacial musculoskeletal disorder.
T-Scan Guided Occlusal Corrections: Why Symptoms Improve
Many cases of unexplained headaches respond dramatically after:

correction of deflective contacts
reduction of disclusion time
restoration of posterior stops
stabilization splint therapy
restoring vertical dimension when needed

This reduces:
muscle overwork
trigger points
TMJ microtrauma
neurogenic inflammation

Clinical observation
In many patients with masseter hypertrophy:
after correction of occlusal overload, hypertrophy reduces over time due to decreased muscle recruitment.
Occlusion + Airway: The Underestimated Link
Does tooth loss affect snoring and OSA? Yes.

When OVD is reduced:
mandible shifts backward (retroposition)
deep bite increases
tongue space reduces
pharyngeal airway space decreases (PAS)
This can worsen:
snoring
airway resistance
OSA risk
Tooth loss is therefore not only cosmetic and functional loss—it can be a sleep health risk.
Facebow and Articulators: Small Step, Huge Impact
Occlusion is 3D.Ignoring jaw relation leads to errors.

Recording is critical:
maxillary relation to Frankfort plane
hinge axis approximation
functional mandibular movements
A facebow transfer helps mount casts appropriately. Selection of a semi-adjustable/fully adjustable articulator improves prosthesis accuracy.
Why CAD-CAM Precision Crowns Are Essential

A crown should replicate:
anatomy
contact points
cusp inclines
guidance
proper occlusal scheme
Poor crowns lead to:
premature contacts
broad occlusal tables
muscle overload
TMJ instability
Therefore:
✅ Digital CAD-CAM precision crowns
✅ Biocompatible materials (with warranty)
✅ Correct occlusal replication is essential.
Where EMG Strengthens Diagnosis
Surface electromyography (EMG) records muscle activity (microvolts) at rest and function.
It helps:
confirm hyperactivity
evaluate left-right imbalance
document improvement after correction

T-Scan + EMG integration
This is modern evidence-based occlusal dentistry:
occlusal correction is documented
results are measurable
medico-legal documentation becomes stronger EMG Curtesy to Dr Vijay Kumar My Senior
Clinical Message to Patients
If you have:

headaches with no medical cause
jaw tightness
neck pain
facial pain
tinnitus
pain while chewing
repeated crown failure
broken fillings
worn teeth
enlarged jaw muscles
Do not ignore the possibility of occlusal overload and bite imbalance.
Conclusion
Malocclusion is not just crooked teeth. It is a biomechanical imbalance that can disturb:
Muscles
TMJ
Cervical chain
Facial nerves
Airway function
Modern dentistry must move beyond “paper bite checking” into scientific occlusal analysis.
T-Scan guided occlusal diagnosis and correction is one of the most powerful advancements for treating:

occlusion-induced headaches
facial pain syndromes
TMJ disorders
clenching/bruxism overload
masseter hypertrophy
Consultation / Appointment
To evaluate and correct occlusion-related headaches, neuralgias, TMD pains, facial pains, bite collapse, and airway compromise, book your consultation:
Issued in public interest– Dr. S. S. Narayana
Disclaimer
This article is written for educational purposes and to bring awareness among the public, with clinical case study images used only with patient consent. Some images/illustrations may be sourced from public web resources and remain copyrighted to respective owners. We acknowledge and respect original creators. If you own rights to any visual content referenced and do not wish it to appear, kindly contact us and it will be promptly removed. Knowledge is virtue.
References (Scientific)
Okeson JP. Management of Temporomandibular Disorders and Occlusion. 7th ed. Elsevier; 2013.
Manfredini D, Winocur E, Guarda-Nardini L, Paesani D, Lobbezoo F. Epidemiology of bruxism in adults: A systematic review of the literature. J Orofac Pain. 2013.
Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for clinical and research applications. J Oral Facial Pain Headache. 2014;28(1):6–27.
Greene CS. Managing the care of patients with temporomandibular disorders: A new guideline for care. J Am Dent Assoc. 2010.
Dawson PE. Functional Occlusion: From TMJ to Smile Design. Mosby; 2007.
Kerstein RB. Disclusion time reduction therapy with T-Scan in treating chronic myofascial pain. Dent Today. Various publications.
Kerstein RB, Radke J. Clinician accuracy when using articulating paper to locate occlusal contacts. CRANIO. (studies relating to occlusal marking limitations).
Slavicek R. The Masticatory Organ: Functions and Dysfunctions. Gamma Medizinisch-Wissenschaftliche Fortbildungs AG.
Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013.
American Academy of Sleep Medicine (AASM). International Classification of Sleep Disorders (ICSD-3). 2014.
Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med. 2014.
Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and OSA with oral appliances. Sleep. 2006.


Comments